|
| |
|
 |
DRUG TESTING
Frequently Asked Questions |
 |
Q:
What are the common drugs of abuse and how do they work?
A: Alcohol: Alcohol,
while a legal drug, is often abused and habitual use can lead to addiction and
significant physical and psychological health problems. Alcohol is rapidly
metabolized by the liver into its principle chemical components including carbon
dioxide and sugars. Alcohol is within the family of depressant drugs with
symptoms including slurred speech, loss of motor coordination and impaired
judgment. Alcohol is consumed primarily for its psychotic effects which include
a loss of inhibitions and euphoria. Alcohol can only be detected through testing
for a relatively short period due to its rapid metabolization and elimination.
Generally, detectable levels of alcohol intoxication are gone within
6-8
hours. Consequently all alcohol tests must be performed during or shortly after
consumption.
Amphetamine:
(AMP)
Amphetamines are central nervous stimulants whose effects include alertness,
wakefulness, increased energy, reduced hunger and an overall feeling of well
being. Large doses and long term usage can result in higher tolerance levels and
dependence. The most common source for amphetamine are the prescription diet
pills (Phentermine).
Cocaine:
(COC)
Cocaine is made from coca leaves. Its effects include alertness, wakefulness,
increased energy and an overall feeling of euphoria. Cocaine may be smoked,
inhaled ("snorted") or injected. Cocaine can be a very addictive drug.
Cocaine is metabolized by the body into the chemical compound Benzoylecgonine.
Methamphetamine:
(MET or M-AMP)
Methamphetamine is a stimulant drug which is quickly metabolized to amphetamine.
It is used in pill form, or in powdered form by snorting or injecting.
Crystallized methamphetamine is inhaled by smoking and is a considerably more
powerful form of the drug. Some of the effects of methamphetamine use include:
increased heart rate, wakefulness, physical activity and decreased appetite.
Methamphetamine use can cause irreversible damage to the brain, producing
strokes and convulsions, which can lead to death. Ecstasy, a new trendy and
popular drug among teenagers is a refined and processed form of
methamphetamine.
Opiates:
(OPI)
Opiates are any of the addictive narcotic drugs derived from
the resin of the poppy plant.
Opiates
are analgesics (pain reducers) which work by depressing the central nervous
system. They can also depress the respiratory system. Doctors often prescribe
them for severe or chronic pain. Opiates are very addictive, both physically and
psychologically. Use for only a short time normally results in addiction. Some
commonly used opiates are: Codeine, Darvon, Heroin, Methadone, Morphine, Opium,
Percodan, Talwin, Dilaudid and Demerol. Opiates are commonly referred to as
"downers". Opiates can appear in many forms: white powder or crystals; small
white, yellow or orange pills; large colorful capsules; clear liquid and dark
brown, sticky bars or balls. Heroin accounts for the majority of the illicit
opiate abuse.
Some physical indications of opiate use include: extreme loss of appetite and weight, needle tracks or punctures, black and blue marks from "skin popping", scars along veins, cramps, nausea, vomiting, excessive scratching and complaint of itching,
excessive sweating, constipation, raw, red nostrils from snorting,
runny nose, pin-point pupils and watery eyes, reduced vision, drowsiness,
euphoria, trance-like states, excessive thirst, tremors, twitching, unkempt
appearance, strong body odor, irritability, chills; slight hallucinations and
lethargy.
Opiates reduce attention
span, sensory and motor
abilities, produce irrational behavior, depression, paranoia, and other
psychological abnormalities.
Oxycodone
(OXY) Pharmaceutical drugs Percodan, Percocet,
Roxicodone, Oxycontin. While classified as an Opiate, the chemical structure and
metabolite of Oxycodone requires a separate Opiate test with a substantially
higher sensitivity detection level than that of the standard Opiate drug test.
Consequently, a positive test result will not only confirm Oxycodone but other
opiates as well. In this regard the Oxycodone test is not Oxycodone specific but
opiate specific being able to detect Oxycodone/opiate use at the higher
sensitivity level required while the 2000 ng/ml sensitivity level of the
standard opiate test would not detect Oxycodone. Oxycodone is generally
prescribed in oral pill form with the analgesic buffer Acetaminophen.
Acetaminophen, 4'-hydroxyacetanilide, is a non-opiate, non-salicylate analgesic
and antipyretic which occurs as a white, odorless, crystalline powder,
possessing a slightly bitter taste. Its molecular formula is C8H9NO2.
The molecular weight is 151.17. The Oxycodone component is
14-hydroxydihydrocodeinone, a white, odorless, crystalline powder having a
saline, bitter taste. It is derived from the opium alkaloid thebaine. Its
molecular formula is C18H21NO4·HCl.
The molecular weight is 351.83.
Phencyclidine:(PCP)
Phencyclidine hydrochloride (or PCP), also know as "angel dust," is a
hallucinogen. PCP is commonly taken orally, by inhalation, by
"snorting" or by injection. The effects of this drug are unpredictable
and variable. Users may exhibit signs of euphoria, anxiety, relaxation,
increased strength, time / space distortions, panic or hallucination. PCP use
can lead to paranoia and extreme irrational behavior. Once popular, PCP use has
declined dramatically in recent years and is no longer considered a major drug
of abuse.
Propoxyphene
(PPX) Propoxyphene (PPX) is a narcotic analgesic compound bearing structural
similarity to methadone. As an analgesic, propoxyphene can be from 50-75% as
potent as oral codeine. Darvocet™, one of the most common brand names for the
drug, contains 50-100 mg of propoxyphene napsylate and 325-650 mg of
acetaminophen. Peak plasma concentrations of propoxyphene are achieved from 1 to
2 hours post dose. In the case of overdose, propoxyphene blood concentrations
can reach significantly higher levels. In humans,
propoxyphene is metabolized by N-demethylation to yield norpropoxyphene.
Norpropoxyphene has a longer half-life (30 to 36 hours) than parent propoxyphene
(6 to 12 hours). The accumulation of norpropoxyphene seen with repeated doses
may be largely responsible for resultant toxicity.
THC (marijuana):
(THC)
Tetrahydrocannibinol (THC) is an active component in marijuana. Marijuana, a
hallucinogen, is commonly ingested by smoking, but it may also be eaten.
Marijuana may impair learning and coordination abilities. Marijuana is most
commonly the drug of choice among teenagers and young adults. The hallucinogenic
effect of Marijuana can lead to irrational behavior, disorientation, and
paranoia. Low concentrations of THC persists in urine at a detectable
concentration for many days after smoking. Marijuana is the most common
recreational drug of abuse.
Barbiturates:
(BAR) Classified generally as
depressants, barbiturates produce a state of intoxication that is remarkably similar to alcohol intoxication. Symptoms include slurred speech, loss of motor coordination and impaired
judgment. Depending on the dose, frequency, and duration of use, one can rapidly develop tolerance, physical dependence and psychological dependence on barbiturates.
Barbiturate abusers prefer the short-acting and intermediate-acting barbiturates pentobarbital (Nembutal), secobarbital (Seconal) and amobarbital (Amytal). Other short-and intermediate-acting barbiturates are butalbital (Fiorinal, Fioricet), butabarbital (Butisol), talbutal (Lotusate) and aprobarbital (Alurate). After oral administration, the onset of action is from 15 to 40 minutes and the effects last up to 6 hours.
Benzodiazepines:
(BZO) Also classified as
depressants, benzodiazepines are used therapeutically to produce sedation, induce sleep, relieve anxiety and muscle spasms and to prevent seizures. In general, benzodiazepines act as hypnotics in high doses, as anxiolytics in moderate doses and as sedatives in low doses.
Like the barbiturates, benzodiazepines differ from one another in how fast they take effect and how long the effects last. Shorter acting benzodiazepines, used to manage insomnia, include estazolam (ProSom), flurazepam (Dalmane), quazepam (Doral), temazepam (Restoril) and triazolam
(Halcion). Benzodiazepines with longer durations of action include alprazolam (Xanax), chlordiazepoxide (Librium), clorazepate (Tranxene), diazepam (Valium), halazepam (Paxipam), lorazepam (Ativan), oxazepam (Serax) and prazepam
(Centrax). Abuse of Benzodiazepines occurs primarily because of the
"high" which replicates alcohol intoxication. Approximately 50 percent of people entering treatment for narcotic or cocaine addiction also report abusing benzodiazepines.
Methadone:
(MTD) Although chemically unlike morphine or heroin, methadone produces many of the same effects.
Methadone is primarily used today for the treatment of narcotic addiction. The effects of methadone are longer-lasting than those of morphine-based drugs. Methadone's effects can last up to 24 hours, thereby permitting administration only once a day in heroin detoxification and maintenance programs.
Ironically, methadone, used to control narcotic addiction, is a frequently
abused narcotic, often encountered on the illicit market and
methadone has been associated with a number of overdose deaths.
MDMA (Ecstasy):
(MDMA)
Methylenedioxymethamphetamine (Ecstasy) is a designer drug first synthesized in
1913 by a German drug company for the treatment of obesity. Those who take the
drug frequently report adverse effects, such as increased muscle tension and
sweating. MDMA is not clearly a stimulant, although it has, in common with
amphetamine drugs, a capacity to increase blood pressure and heart rate. MDMA
does produce some perceptual changes in the form of increased sensitivity to
light, difficulty in focusing, and blurred vision in some users. Its mechanism
of action is thought to be via release of the neurotransmitter serotonin. MDMA
may also release dopamine, although the general opinion is that this is a
secondary effect of the drug. The most pervasive effect of MDMA, occurring in
almost all people who have taken a reasonable dose of the drug, is to produce a
clenching of the jaws. Symptomatic and biological responses to MDMA are similar
to those produced by methamphetamine.
Nicotine:
(COT)
Most
experts and healthcare professionals agree that nicotine is unquestionably the
most addictive drug in use today. The principle source of nicotine is tobacco
products. Tobacco smoking or chewing results in the absorption
of nicotine through the lung and buccal/nasal epithelium, after which nicotine is
metabolized into 20 metabolites excreted in urine including
the primary metabolite Cotinine. Cotinine metabolite is the primary marker for
nicotine tests and tobacco use screening.
Smoking
has been confirmed as contributory factor to throat and lung cancer as well as
other major health problems including heart disease. Chewing tobacco or use of "snuff", the
refined powder version of tobacco has been found to contribute to the
development of oral cancers and tumors including other major diseases of the mouth and oral tissues.
Tricyclic antidepressants, (TCA)
Tricyclic antidepressants have been prescribed since the 1950s for depression
and compulsive disorders. Until recently TCAs were the
primary choice of physicians for the vast majority of people with major
depressive disorders. Ironically TCAs are often prescribed
for symptomatic treatment of drug addiction and withdrawal and in particular,
alcoholism. Tricyclic antidepressants work by raising
the levels of serotonin and norepinephrine in the brain by slowing the rate of
reuptake, or re-absorption, by nerve cells. Usually TCAs are taken over an
extended period as results from the drugs are gradual. Because of the
possibility of causing serious cardiac complications, TCAs can be lethal if
misused at high doses. Abuse of TCAs can be the result of fear of relapse rather
than any psycho-pharmacological effect however the potential for TCA abuse is
well established, since the drugs have clearly defined euphoric psychological
and stimulatory physiological action in cases of chronic usage. Generic and brand names
of the tricyclic antidepressants include
Adapin, Amitriptyline, Amoxapine, Asendin, Desipramine, Doxepin, Elavil,
Imipramine, Ludiomil, Maprotiline, Norpramin, Nortriptyline, Pamelor,
Pertofrane, Protriptyline, Sinequan, Surmontil, Tofranil, and Vivactil. Any
comprehensive drug screening program should include a TCA panel.
Q:
What are the so-called Date Rape Drugs and how do they work?
A: Rohypnol and GHB. Rohypnol is a sleeping pill marketed by Roche Pharmaceuticals.
The drug is a very potent tranquilizer similar to Valium, but much, much stronger. Rohypnol falls in the general drug class of Benzodiazepines. Rohypnol like all benzodiazepine drugs produces a sedative effect, amnesia, muscle relaxation and a slowing of psychomotor responses. The drug is often distributed on the street in its pharmaceutical packaging which makes it appear legitimate and legal. Rohypnol is reportedly sold for $2.00 to $4.00 per tablet. Originally, illicit use of Rohypnol was reported in Europe in the late 1970's while first reports of Rohypnol use in the United States began in the early 1990's.
Rohypnol side effects begin approximately 20-30 minutes after taking the drug and peak within two hours. The half life of system induced Rohypnol, dependent on dosage is up to 8 hours. Symptoms of Rohypnol use include decreased blood pressure, black outs (memory loss), disorientation, blurred vision, aggressive behavior,
loss of inhibitions, and extreme anxiety. Rohypnol is known as a rape drug because perpetrators reportedly slip it into a victim's drink causing them to blackout. Rohypnol takes away a victim's normal inhibitions, leaving the victim helpless and blocking the memory of a rape or
assault. Rohypnol would test positive for
Benzodiazepines in a typical lateral flow urine test device.
It must be noted, however, that because the half life of Rohypnol is relatively
short (< 8 hours), testing would have to take place within a few hours of
ingesting of the drug.
GHB (Gamma-Hydroxybutyerate) Originally developed as an anesthetic, GHB is a naturally occurring 4-carbon molecule sold in powdered, liquid or capsule form.
GHB usually is tasteless, but may be recognized at times by a salty taste. GHB was formerly sold by health-food stores and gyms as a sleep aid, anabolic agent, fat burner, enhancer of muscle definition and natural psychedelic. GHB was first synthesized in 1960 by a French researcher. It has been used in Europe as a general anesthetic, a treatment for insomnia and narcolepsy, an aid to childbirth and a treatment for alcoholism and alcohol withdrawal syndrome. In the last few years it has been gaining popularity as a "recreational" drug offering an alcohol-like, hangover free "high" with possible
pro-sexual effects (dis-inhibition often occurs and inhibitions are extremely suppressed).
GHB side effects are usually felt within 5 to 20 minutes after ingestion and they usually last no more than two to three hours. The effects of GHB are unpredictable and very dose-dependent. Sleep paralysis, agitation, delusions and hallucination have all been reported. Other effects include excessive salivation, decreased gag reflex and vomiting in 30 to 50 percent of users. Dizziness may occur for up to two weeks post ingestion. GHB can cause severe reactions when combined with alcohol, benzodiazepines, opiates, anticonvulsant and allergy remedies.
Presently there are no lateral flow urine tests for GHB.
Q: What is
my teenager likely to call these drugs?
A: Common street names for
drugs:
|
Amphetamine
|
Speed,
amp, bennies, black beauties, chalk, uppers, hi, speed balls, beans,
hiballs, beenie babies, eve
|
|
Methamphetamine
|
Crystal,
meth, ice, glass, speed, icebergs, bergs, ecstasy, MDEA,
|
|
Cocaine
|
Coke,
crank, snow, flake, crack, blow, rock, line, snuff, sugar, snort, stones
|
|
Marijuana
|
Pot,
weed, herb, bud, MJ, doobie, reefer, joint, blunts, grass, rope, hemp,
roach
|
|
Phencyclidine
(PCP) |
Angel
dust, sherms, star dust, magic dust, dust, silver/gold glitters
|
|
Opiates
(heroin) |
Horse,
smack, hairy hombre, H, scag, jones, fix
|
|
Barbiturates Benzodiazepines
|
Downers, uppers, highway, lows,
reds, barbs, trangs |
|
GHB (Gamma-Hydroxybutyerate)
|
G, Liquid X, Liquid E, Scoop, Soap,
Gook, Grievous Bodily Harm, Georgia Home Boy, Natural Sleep-500, Easy
Lay or Gamma 10 |
|
Rohypnol
|
roofies, Roche, R-2, rib and rope,
rophies |
Q:
How long after cocaine use can it be detected in the urine?
A: Cocaine is excreted in the urine primarily as benzoylecgonine in
a short period of time. Benzoylecgonine can be generally detected for 24 to 60
hours after cocaine use or exposure. Exact clearance rate times can't be
determined since the metabolic rate is individualized depending on weight and
other factors.
Q:
In general, what are the drug detection periods for the most abused drugs and
how long after use can drug tests detect drug presence
or use?
A: Drug of abuse
testing by blood, urine, saliva or any other method (except
forensic hair analysis) is designed only to detect whether or not a
specific drug or drug metabolite is present at the time the
test is performed. While there are very broad estimates as to how long a
particular drug may have been in the system, no drug test, regardless of method,
is intended to include a time variable. Many factors unique to the individual
being tested determine the actual half-life of the particular drug including
such variables as age, weight, body fat index, sex,
metabolic rate, overall health and amount of drug
consumed over what period of time. Therefore, no conclusions can be drawn
as to when a particular drug was taken or how much was consumed with any type of
drug of abuse test. The following chart illustrates typical drug detection periods.
For reasons noted, the
range stated is necessarily broad. Generally however, chronic
use of high potency drugs by individuals with a high body fat count, low
metabolism rate (older) and in poor general health will place drug clearance
periods at the higher range. To re-emphasize, it should be clearly understood that drug
tests are not intended to determine when drugs
were used, only whether the drug screened for is present at the time the test is
performed. If it is desirable to screen for
historical drug use, a forensic laboratory hair
analysis test is available that will screen for illicit drug use up to 90
days dependent on hair sample length. It should also be clearly understood that complete
abstinence from the target drug is required from the start of the
"minimum" to the end of the "maximum" detection
period to clear the user's system completely.
|
TYPICAL DRUG DETECTION/CLEARANCE TIMES |
|
Target Drug |
Minimum |
Maximum |
|
Alcohol |
0-4 hours |
<=6-8 hours
|
|
Amphetamines |
2-7 hours |
2-4 days |
|
Anabolic Steroids |
4-6 hours |
Oral: 2-3 weeks / Injected: 1-3 months (Naldrolene 8 months+) |
|
Barbiturates |
2-4 hours |
Short acting type (Alphenal, Amobarbital, Allobarbital,
Butethal, Secobarbital) 1-4 days.
Long acting type (Phenobarbital, Barbital) 2-3 weeks or longer |
|
Benzodiazepines |
2-7 hours |
Infrequent user: 3 days / Chronic user: 4-6 weeks |
|
Cannabinoids (THC-Marijuana)* |
6-18 hours |
*Infrequent user: up to 10 days
/
Chronic user:30 days or longer |
|
Cocaine Metabolite |
1-4 hours |
2-4 days |
|
LSD |
2
hours |
1-4 days |
|
Mescaline |
1-2 hours |
2-4 days |
|
Methadone |
2
hours |
2-6 days |
|
Methamphetamines |
1-3 hours |
2-4 days |
|
Methaqualone |
3-8 hours |
Up
to 10 days |
|
MDMA (ecstasy) |
1
hour |
2-3 days |
|
Nicotine (Tobacco)** |
4-6 hours |
**Infrequent
user: 2-3 days / Chronic user: 7 to 14 days |
|
Opiates (Heroin, Morphine, Codeine)
|
2
hours |
2-3 days |
|
Oxycodone |
1 hour |
1-2 days |
|
Phencyclidine (PCP)* |
5-7 hours |
*Infrequent user: 6-8 days / Chronic user: 21-28 days+ |
|
Propoxyphene |
4-6 hours |
1-2
days |
|
Psilocybin (Mushrooms) |
2
hours |
1-3 days |
|
Rohypnol |
1
hour |
< =8 hours |
|
GHB |
1
hour |
< =8 hours |
|
Tricyclic
Antidepressants (TCA) |
8-12 hours |
2-7 days |
|
* THC and PCP in
particular are stored by the system in the fatty lipid tissue and are
gradually released into the blood stream until cleared. For chronic
users with a high body fat count, this process can take several weeks.
** Nicotine is one of the most addictive drugs known. Consequently most
users of nicotine are chronic users by default. Nicotine consumption
includes all forms of the drug including tobacco, snuff, transdermal
patches and gum. |
Q: If a drug test is positive, can you determine how long ago the drug was taken
and over what period of time?
A: No. Drug of abuse testing by blood, urine, or saliva can only detect
whether or not a specific drug or drug metabolite is present at the time the
test is performed. While there are very broad estimates (see chart above) as to
how long a particular drug may have been in the system, no fluid based drug
test, regardless of method, is intended to include a time variable. Many factors
unique to the individual being tested determine the actual half-life of the
particular drug including such variables as age, weight, sex, metabolic rate,
overall health, amount of drug consumed over what period of time, etc.
Therefore, no conclusions can be drawn as to when a particular drug was taken or
how much was consumed with these types of drug of abuse tests. A forensic hair
core analysis for drugs can be utilized to determine historical drug use up to
90 days. See the Hairconfirm™ forensic drug testing
service.
Q:
I am taking a prescription medication. Will this particular
medication test positive on a drug test?
A:
There are literally hundreds of brand name and generic drugs
being prescribed today. If you have a question on a specific prescribed
medication, you will need to know the general classification of that medication
to determine if it will test positive on any of the specific drug test panels,
ie: opiates, amphetamine, methamphetamine, benzodiazepines, barbiturates etc.
For general classifications on prescription drugs you can either ask your
pharmacist or go online to http://www.rxlist.com
and enter the name of the prescription drug to determine it's general
classification and pharmacology.
Q: What are the effects of sample dilution or adulteration and how are these
tested for?
A: The most common method of sample manipulation to avoid a positive drug screen
is dilution. Other forms of sample adulteration are the in vitro addition of
adulterants or additives into the specimen sample to destroy the chemical
reaction properties of lateral flow. point of use, drug tests. Common practice
is to pre-test the sample for dilution or adulteration using a
sample
validity test. The chart below shows the effect that dilution,
adulteration or substitution has on standard drug screens.
|
Specimen Validity/Adulteration Testing |
|
Validity Marker |
Commercial Product |
Method of Introduction to Urine |
Mode of Action |
|
Creatinine |
H˛O |
In vivo or in vitro.
Creatinine is always present in normal human urine however abnormally low or
absent levels would indicate diluted or substituted non human samples.
|
Creatinine is excreted from the body at a
constant rate and there are expected values for creatinine in urine. When
abnormally large quantities of fluids (H˛O) are consumed in vivo the urine
is diluted and creatinine levels are substantially reduced as are other
detectable chemical markers including drugs and their metabolites.
Alternatively a sample donor may attempt to compromise a test result by
adding water to the urine sample (in vitro) to dilute drug concentrations.
Creatinine levels are usually checked in conjunction with Specific Gravity
to screen for diluted or substituted specimens.
|
|
Nitrites
Oxidants |
Klear, Whizzies
UrineLuck |
In vitro. Donor adds
potassium nitrate to the urine specimen |
Nitrates are oxidizing
agents that attack the drug or drug metabolite molecules when present at
high concentrations. The primary effect of nitrates is to interfere with
antibody binding in lateral flow tests and GC/MS confirmation testing of
cannabinoid positives. Specimens with abnormally high nitrate levels should
be considered as suspect. |
|
pH |
N/A |
In vivo by ingestion of
substances that would change the urine pH values to outside the normal range
( virtually impossible) or in vitro when the the donor adds a acidic or
caustic agent (bleach) to the the sample to grossly modify the pH.
|
The pH of the sample may
influence or compromise the enzymatic and antibody reactions in lateral flow
drug tests. An extremely high (>9.5) or low (<3.0) pH may depress the
enzymatic rate. Also the chemical stability of the drug or drug metabolite
may be compromised resulting in a false negative or negative test reaction
requiring a retest with a fresh specimen.
|
|
Specific Gravity |
H˛O |
In vivo. Donor consumes large quantities of
liquids (H˛O) or in vitro, the donor adds fluid (H˛O) to the urine specimen.
|
Abnormally low readings
of Specific Gravity generally indicate a diluted sample especially when
creatinine levels are also low. |
|
Glutaraldehyde |
UrinAid
ClearChoice |
In vitro. Donor adds
cleansing agents containing Glutaraldehyde. |
Glutaraldehyde interferes with the enzymes
used in some lateral flow drug tests resulting in a false negative or
invalid test result. |
|
lgG Hormone |
N/A |
Dilution or substitution
with non human urine. |
Human lgG is exclusive
to human body fluids and is not present in any other liquids or animal
urines. Consequently, if lgG is not present or cannot be detected in a urine
sample, the sample is either non human urine, or has been diluted or
otherwise contaminated by addition of an adulterant. |
Q:
Unexpected
results or test failure. What is the likelihood that the test device is
defective?
A. 98% of the time, unexpected test results
or failure to obtain test results is the result of user error. Failure to follow
instructions, inadequate sampling, device contamination, failure to use a timer
or other user related factor. In-vitro, lateral flow chromo-graphic tests while
simple to use still require certain basic testing disciplines. Unfortunately
persons unfamiliar with these disciplines often ignore the test instructions or
cautions expecting the test device to be accurate regardless of how it is used.
Additionally, the stringent quality control checks and required random sampling
methods mandated by the governmental regulatory authorities during the production process make
the likelihood of receiving a defective test device extremely remote.
Q:
What is the difference between heroin and morphine?
A: Heroin, morphine and codeine are opiates derived from the resin
of the opium poppy. Heroin is quickly metabolized to morphine. The body also
changes codeine (used in some cold medicines) to morphine. Thus, the presence of
morphine in the urine indicates heroin, morphine and/or codeine use.
Q:
What does THC mean?
A: THC is an abbreviation for 11-nor-delta9 Tetrahydrocannibinol-9-carboxylic acid, the primary metabolite of Marijuana. Marijuana is a
hallucinogenic agent derived from the leaves, flowers or seeds of the hemp
plant. In general, the production and "curing" of the marijuana plant
into its useable form closely resembles that of tobacco. Marijuana
is almost always smoked and inhaled into the lungs where it is quickly
metabolized (or changed) by the body into
11-nor-delta-9-tetrahydrocannabinol-9-carboxylic acid which is excreted in the
urine.
Q. What is the difference
between morphine, heroin and codeine?
A: Chemically, nothing. All three of these drugs are derived from
opium or the opium chemical structure and are in the Opiate class of drugs. The
difference is primarily in the manner in which opium is refined or synthetically
manufactured and the form and method of delivery.
Q:
Why is there a separate test for Oxycodone if Oxycodone
is an Opiate?
A: Oxycodone (Percodan, Percocet, Roxicodone, Oxycontin)
are synthetically manufactured opiates meaning they are not directly refined
from the opium poppy resin source. While the chemical chains are similar,
detection of synthetic opiate drugs requires a lower sensitivity detection level
than that established for non synthetic opiates.
Q:
What is the difference between Methamphetamine and Amphetamine?
A: Both amphetamine and methamphetamine are potent symphathominetic
agents. Methamphetamine is the parent drug. It metabolizes (or changes) into
amphetamine in the body. Methamphetamine and/or amphetamine are excreted in the
urine. A positive result for Amphetamine can also be interpreted as a positive
test for methamphetamine.
Q:
What is Ecstasy?
A. Ecstasy (MDMA) has recently become a popular recreational drug among
teenagers and young adults. Ecstasy is refined processed form of amphetamine with a
chemical structure closely resembling methamphetamine. Any test with a target
screen for methamphetamine should detect Ecstasy although a
MDMA specific screen in preferred.
Q:
What does PCP mean?
A: PCP is an abbreviation of phencyclidine which is an
arylcyclohexylamine. One street name is "angel dust".
Q:
What drugs could interfere and cause a positive morphine
(opiates) test?
A: Codeine and Meperidine are structurally related to morphine
therefore causing positive results. Codeine is a commonly prescribed pain
medication and is also the active ingredient in some prescription cough
medicines. These forms of codeine can also be addictive and abused.
Q: What are the drug test sensitivity cut-off levels established
as standard by the NIDA, WHO and SAMHSA for the different drugs of abuse?
A: The table below indicates the
standardized threshold concentration levels for lateral flow immunoassay tests
established by the international regulating authorities. These levels are
reviewed and updated periodically to conform to new data on drug development,
technology and testing statistics. Concentration is expressed in nanograms per
milliliter solution.
|
Symbol |
Target Drug/Metabolite |
Conc |
|
THC |
marijuana/cannabis |
50 ng/ml |
|
COC |
cocaine/benzoylecgonine |
300 ng/ml |
|
PCP |
phencyclidine |
25 ng/ml |
|
OPI |
opiates/morphine |
2000 ng/ml |
|
MET |
methamphetamine |
1000 ng/ml |
|
MDMA |
Ecstasy |
500 ng/ml |
|
OXY |
Oxycodone |
100 ng/ml |
|
AMP |
amphetamine |
1000 ng/ml |
|
MTD |
methadone |
300 ng/ml |
|
BAR |
barbiturates |
300 ng/ml |
|
BZO |
benzodiazepines |
300 ng/ml |
|
TCA |
tricyclic antidepressants |
30 ng/ml |
|
PPX |
Propoxyphene |
300 ng/ml |
Q:
What should I do if there is no control line appearing when I perform the test?
A: Repeat the test, carefully following the written procedure.
The most common cause for a control line not developing or appearing is failure to add
sufficient urine sample to complete full migration through the test panels.
98% of reported incidents regarding unexpected results, lack of a control line
or test integrity are the result of user error or test contamination at the
point of testing.
Q:
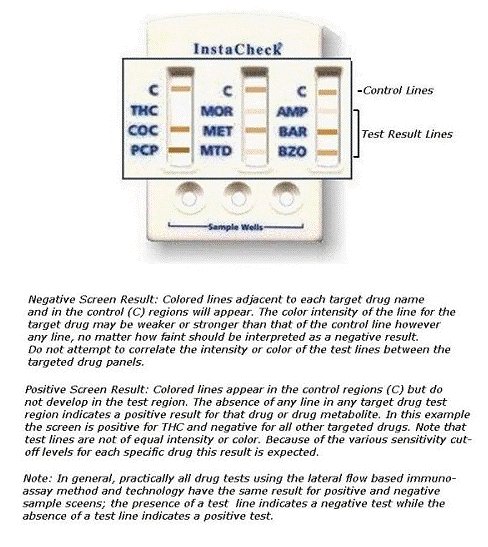
How does the result window appear if the results are negative?
A: Two colored bands will appear, a control
band and a test band on the strip next to the target drug.
See Illustration Sheet
Q
How does the result window appear if the results are positive?
A: Only one band, the control band will appear
and no band will develop when the target drug is present.
See Illustration Sheet
Q:
What do I do if results show a very faint line?
A: Any very faint line on the test region could indicate that the
drug in the sample could be near the cut-off level for the test. However, any line in the test area, no matter how faint, should be interpreted as a negative test. Perform a second test or send the specimen to a laboratory to obtain quantitative results. If laboratory confirmation is desired for uncertain or positive results
consider testing with the "At Home"
QuickScreen Pro Drug Test Kit
which includes laboratory confirmation
of positive results. For initial screening purposes, a faint line
in the test area should always be interpreted as a negative test.
Q:
How long can the urine specimen be stored before testing ?
A: Specimens can be stored in refrigerators at 2 to 8° C for up to
two (2) days (48 hours) or frozen at 0° C, before testing. However, it is
strongly recommend testing the sample as soon as possible after collection.
Q
Will commonly ingested substances such as vitamins, penicillin, aspirin,
caffeine and acetaminophen (Tylenol), affect the results?
A: No. The tests are drug and drug metabolite
specific. Because these commonly ingested substances are chemically and structurally
different after metabolized by the body from the drugs being tested for, they
will under most circumstances not interfere with or compromise test
results.
Q:
What will the control region look like if the test is working ?
A: The control line should always appear regardless of the presence
of drugs or metabolites. If the control line does not appear then all results
are invalid.
Q:
My teenager tests positive for THC but claims exposure to "second hand
smoke". Is this possible?
A: No. Urine concentrations of THC above the cutoff sensitivity level of the
test, or a positive result, are not possible by exposure to second hand smoke.
Q: My teenager has a
positive test for opiates but claims eating poppy seed bagels or other food
products containing poppy seeds. Can this happen?
A:
If the sensitivity cutoff level of the test is the revised
standard of 2000 ng/ml OPI, this is not possible.
Sensitivity standards were raised in the year 2000 from 300 ng/ml to 2000 ng/ml OPI to
eliminate the possibility of false positive results that were possible from
consumption of large quantities of poppy seeds or poppy seed paste at the lower
sensitivity level.
Q.
What different types of Drug Tests are there?
A: Many. Please see the drug tests page
or select the button below.
|





{kind=link}